



Stomach Acid Is Critical For Health
Unpacking the Great Acid Blocker Scam

Story at a Glance
•Many pharmaceuticals on the market are automatically given to large numbers of patients despite the harms of these medications often greatly outweighing their benefits.
•One of the worst offenders are the acid suppressing medications, and their overprescription goes hand in hand with widespread medical blindness to the critical functions of hydrochloric acid throughout the body, the symptoms of low stomach acidity (e.g., many autoimmune disorders), and the actual causes of acid reflux.
•Since the stomach needs to be able to let food in but stay closed while digesting it, its opening (the LES) is pH sensitive and will close when sufficient acid is detected. Because of this, reflux is frequently due to insufficient stomach acid (the production of which declines with age) which causes the remaining acid to leak out into the esophagus. Treating reflux by eliminating all acid causes the LES to stay open, and as a result, hooks patients on the drugs since the moment any acid comes back, it will leak out and cause heartburn.
•A chronic small leak of stomach acid can create many different issues in the ears, nose, and throat (e.g., allergies, coughs, and sinusitis).
•A variety of safe and non-invasive approaches exist to address the wide range of complications from acid reflux and dysfunctional stomach acid production.
Note: due to how many people have been affected by the great acid reflux scam, I revised this article (which was one of the most popular I’ve posted here).
One of the more depressing parts of being an awake physician in the medical system is reading the drug lists of the patients you see and realizing how many prescriptions they are on that do not benefit them, and in many cases harm them. Presently, 66 percent of U.S. adults are estimated to have at least one prescription and on average, they have nine prescriptions filled per year (which can include renewals of an existing one).
Since doctors are extremely reluctant to terminate existing prescriptions, this creates a scenario where people get placed on more and more drugs as they age (some of which are for treating the side effects of other drugs they are taking).
This situation is even worse for the elderly, who have more time to be put on an increasing number of medications, and due to their altered physiology, are also the most vulnerable to the harmful effects of those medications. For example, from 2009-2016, after two billion office visits were assessed, it was found that for adults over 65, 65.1% were on two or more drugs, 48.9% were on four or more, and 36.8% were on more than five (with the highest use occurring in the oldest Americans).
One of the best illustrations of the problem came from a study that compared 119 disabled elderly adults living in nursing homes to 71 matching controls. These patients (on average, were on 7.09 medications) were screened for which of their medications clearly met the existing criteria for being discontinued (on average 2.8 per patient). After those medications were discontinued in the test group, when compared to the controls who remained on all of their existing prescriptions, it was found that:
•The death rate dropped by 23% (in one year, 45% of the control group died, whereas 21% of the test subjects died).
•The annual rate of hospital referrals dropped by 18.2% (30% of the controls vs. 11.8% of the study).
•Not surprisingly, there were also significant cost savings from withdrawing the unneeded medications.
In short, doing nothing except terminating some of the most egregious prescriptions for our elders (who often lack the autonomy to refuse their prescriptions) resulted in a 23% reduction in their death rate. When you consider that many of these drugs are approved for much smaller reductions of the death rate, and that they frequently have a variety of other concerning side effects (e.g., triggering dementia), the absurdity of this situation (e.g., that this pivotal study never changed how we practice medicine) becomes apparent.
For example, almost everyone is put on statins—especially as they get older. Yet in trials evaluating statins, for instance, their effect on 50-75 year old patients’ risk of heart disease, statins caused a 0.4% reduction in the annual risk of a major cardiovascular event (most of which are not fatal) and no benefit in the overall death rate. Likewise, according to the existing trials (which are almost certainly biased to favor the pharmaceutical companies funding them), it was found on average that taking a statin for five years would increase your expected lifespan by three to four days. In contrast, statins are notorious for causing adverse effects which affect at least 20% of recipients. These effects include cognitive impairment and dementia, personality changes, loss of sensation throughout the body, and significant muscle weakness or muscle aches.
This seems absurd until you also consider that statins are also one of the most profitable drug markets in existence.
Note: a more detailed summary of the great statin scam and the tragic adverse effects of statins can be found here.
The Worst Drugs on The Market
A frequent question I receive is what the most harmful medications in America are. Prior to the COVID-19 vaccines (which I feel have earned that distinction), there were two ways I interpreted that question.
Which medications are frequently prescribed to everyone, often provide minimal benefit, and cause actual harm you frequently see in practice?
Which medications are highly toxic and have more narrow uses, but are nonetheless frequently given to patients in many cases where the harms of doing so far exceed any possible benefit?
In regards to the first interpretation, almost every integrative physician I’ve ever asked for their top 5 has listed the following:
•Proton pump inhibitors (PPIs—the most potent acid blocker and focus of this article)
•SSRI antidepressants (e.g., Prozac)
•Statins
•NSAIDs (e.g., Ibuprofen)
Note: they’ve also argued birth control pills, Tylenol, benzodiazepines (e.g., valium), corticosteroids, and flu shots also belong on the above list. Likewise, opioids used to always be on it, but now that the government has gone in the opposite direction and curtailed their prescribing, so they are no longer widely distributed and hence no longer can be in the first category.
In regards to the second interpretation, there are many more answers, but some of the most common ones include:
•Anti-psychotic meditations (used for a wide variety of mood disorders)
•Accutane (used for acne)
•Ciprofloxacin and other fluoroquinolone antibiotics
•Finasteride (commonly used for hair loss)
•Gadolinium (this is used as a contrast agent for MRIs)
•Gardasil (the HPV vaccine)
•Lupron (which amongst other things is used as a puberty blocker)
Note: as the above links show, I’ve gradually been able to cover the key issues with each of these classes of drugs, but I still have a ways to go.
In sales, a common practice is to start with a free or low cost item, and then from the pool of people who get it, use their investment to sell them a moderately priced item, and then from the pool of those buyers, sell a more expensive item and so forth. This business practice, in turn, is known as creating “sales funnels.”
Frequently, with the above drugs, I see a variety of sales funnels. For instance, adolescent girls are frequently put onto birth control pills by their pediatricians (e.g., this survey found 54% of women aged 15-19 had used the pill)—often for reasons unrelated to sex (e.g., painful periods or PMS in a twelve year old).
Birth control pills, in turn frequently cause significant mood swings and mood alterations (e.g., a large study detected a 130% increase in the rates of depression during the first two years of using the pill), which often leads to these new mood disorders being “treated” with an SSRI antidepressant (which now more than 10% of teenage girls are on). In turn, one of the more common side effects of SSRIs are other new psychiatric disorders (bipolar I is the most common) which are then treated with an antipsychotic (or another mood stabilizer).
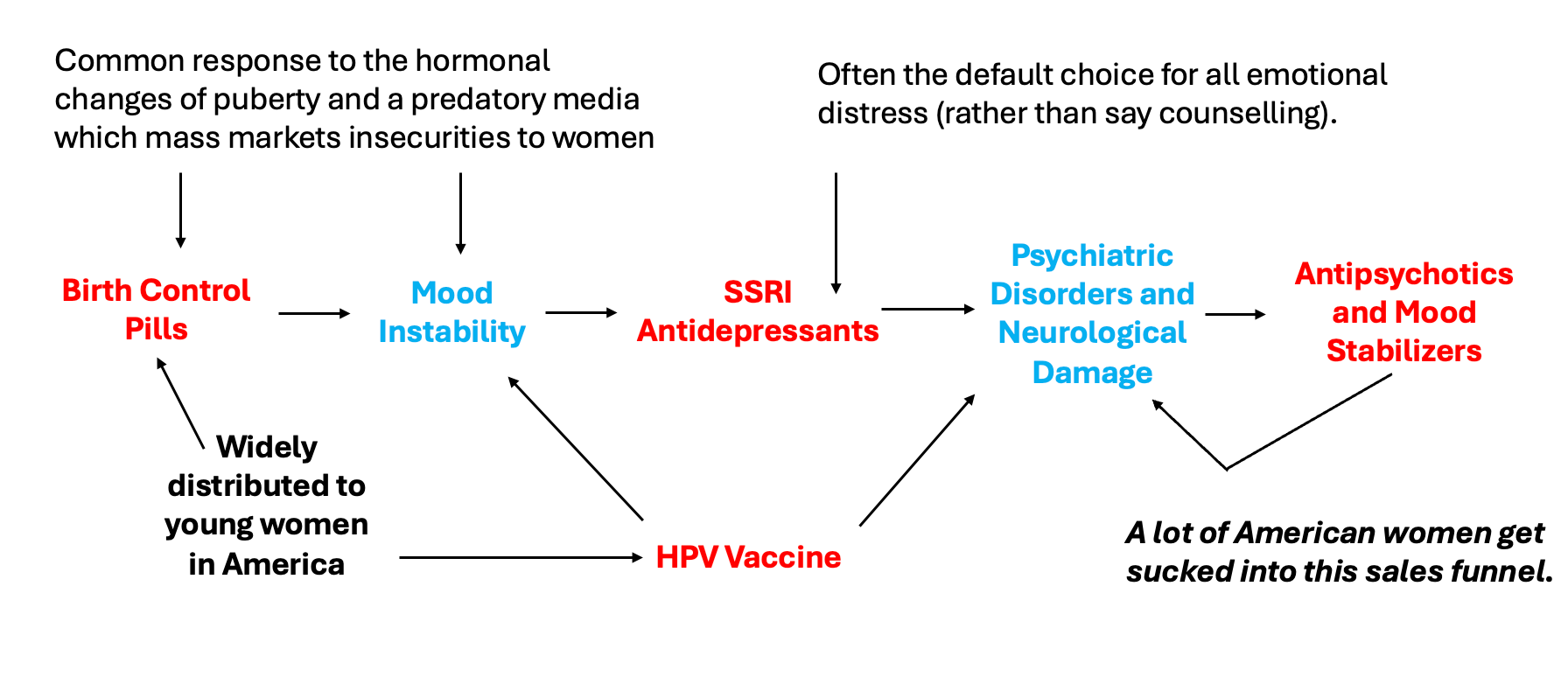
As a result, I often meet young women who went through this sales funnel in their adolescent years and now are on damaging antipsychotics. Additionally, I’ve also spoken to a few people who had been on this pipeline and said the neuropsychiatric damage they developed from the HPV vaccine ultimately tipped them over the edge (which then required taking an antipsychotic which frequently caused even more chronic psychiatric and neurological issues for them).
As you might guess, I am not a fan of this business model, and one of my goals here is to gradually go through why each of these drugs can cause so many problems.
Translational Medicine
Since medicine is supposed to be “science based,” a recurring question is why the most important scientific discoveries are never adopted into clinical practice, or if they are, it often takes years if not decades to be (this is what the discipline of translational medicine seeks to address).
When I first started my medical education, a mentor told me:
The medical profession has always been remarkably conservative in adopting new ideas. Try not to get frustrated if they won’t consider the evidence you present to them.
In turn, in this publication, I’ve tried to gradually review examples of the medical profession's widespread refusal to consider critically important evidence that was being presented to them. By doing so, I’ve hoped to show how this behavior is the norm rather than the exception so each of you can better understand why there has been such a steadfast rejection of science throughout the pandemic.
For example, I am a long time fan of Dr. Mercola (I’ve read his website for decades). A major reason I’ve read it is that Mercola has repeatedly presented ideas (with compelling science to support them) about medicine and health that the medical community rejected. Over and over I’ve seen those ideas be accepted as self-evident truths years later by my profession (e.g., Dr. Mercola correctly predicted that Vioxx would be a disaster).
Yet, despite Mercola having the most read natural health website in the world (leading to many patients demanding the possibilities he puts forward and many physicians adopting his advice), alongside Mercola’s ability to clearly prove his ideas with existing science, the medical profession still has taken years if not decades to accept those ideas. Mercola’s example illustrates how powerful the barriers to translational medicine are. Likewise, consider this Congressional testimony from an FDA scientist who repeatedly tried to get the FDA to pull Vioxx (which sadly forecast precisely what would happen with the COVID vaccines twenty years later):

Go paid at the $5 a month level, and we will send you both the PDF and e-Pub versions of “Government” - The Biggest Scam in History… Exposed! and a coupon code for 10% off anything in the Government-Scam.com/Store.
Go paid at the $50 a year level, and we will send you a free paperback edition of Etienne’s book “Government” - The Biggest Scam in History… Exposed! OR a 64GB Liberator flash drive if you live in the US. If you are international, we will give you a $10 credit towards shipping if you agree to pay the remainder.
Support us at the $250 Founding Member Level and get a signed high-resolution hardcover of “Government” + Liberator flash drive + Larken Rose’s The Most Dangerous Superstition + Art of Liberty Foundation Stickers delivered anywhere in the world. Our only option for signed copies besides catching Etienne @ an event.
So what are some of the ways to address GERD without using PPI's?
Lupron is POISON ☠️ & leaves majority of its users permanently disabled by side effects … 😐😐😐. .. it should be banned for ALL uses immediately